Calcium homeostasis
- N Engl J Med. 2007 Jul 19;357(3):266-81.
- Clin J Am Soc Nephrol. 2010 Jan;5 Suppl 1:S23-30.
- Clin Chem. 1999 Aug;45(8 Pt 2):1347-52.
- Calcium is found primarily in bone (99%), blood and ECF.
- The overall goal of calcium homestasis is to maintain biologically active ionized [Ca] within a narrow acceptable range (1.1-1.4 mmol/L) in order for critical functions such as signal transduction, neuronal activation and muscle contraction to work. These concentrations are tightly regulated by hormonal mechanisms to avoid acute and chronic complications.
Vitamin D synthesis, metabolism and actions
- Ergocalciferol (vitamin D2) and cholecalciferol (vitamin D3) are found in plant and animal sources respectively and absorbed via the intestines. (See figure 1 for activation details)
- Inactivation occurs by further hydroxylation by vitamin D-24 hydroxylase, induced by 1,25(OH)2D itself, producing calcitroic acid which is excreted in bile and urine.
- End organ effects: Vitamin D works to correct hypocalcemia via several mechanisms including: (i) increased uptake of calcium from the intestinal lumen, (ii) calcium reabsorption in the distal convoluted tubules (DCT) in nephrons, (iii) stimulating osteoblasts to secrete RANKL, thereby activating osteoclasts to resorb bone to raise serum calcium levels.
- Vitamin D also suppresses PTH production.
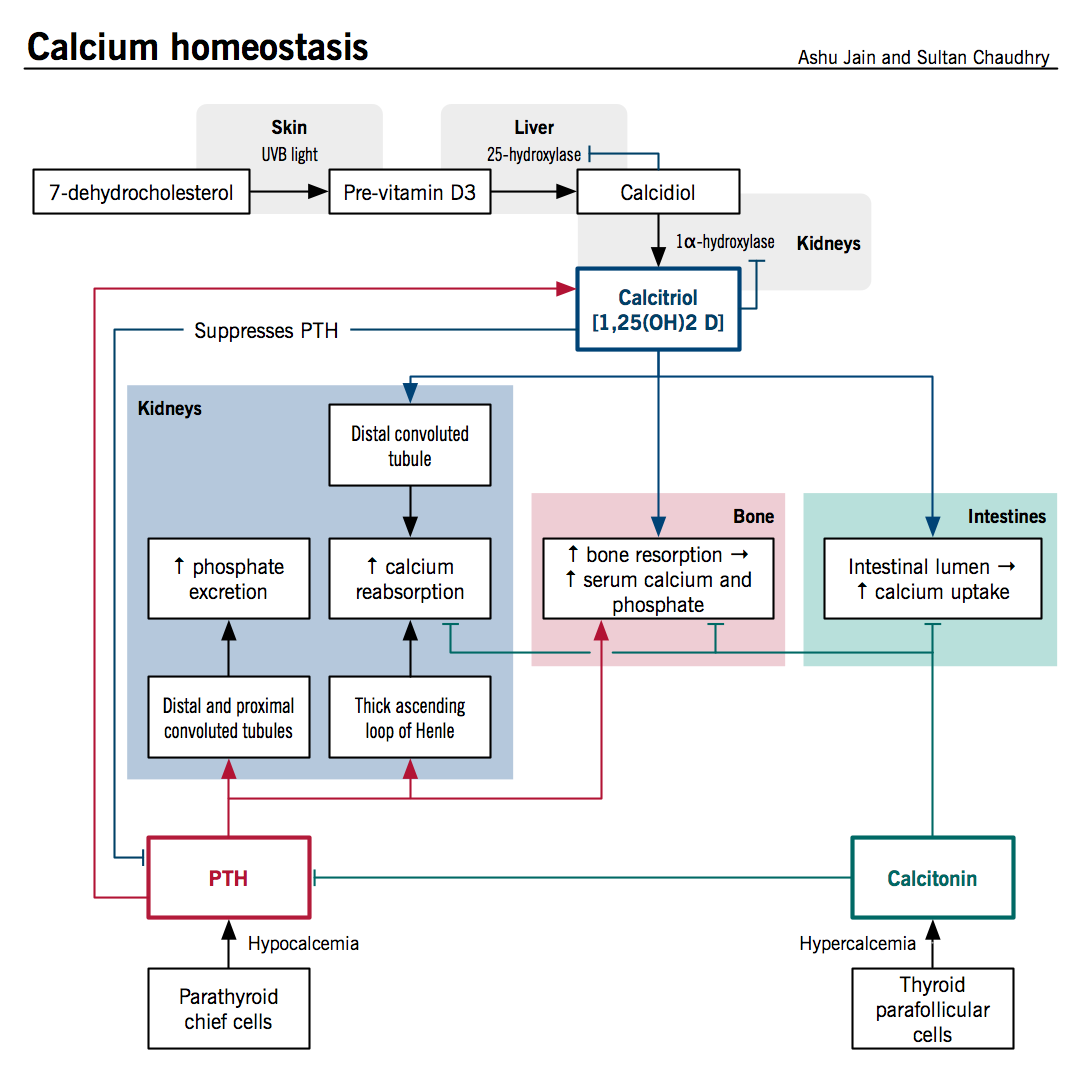
Figure 1: Calcium homeostasis is a process controlled by chiefly by hormones vitamin D and PTH. Vitamin D enters circulation via synthesis in the skin or intestinal absorption and is subsequently converted to its active form, 1,25(OH)2D via separate hydroxylation processes in the liver and kidneys. Both 25(OH)D and 1,25(OH)2D are regulated by classical negative feedback. PTH acts to increase serum calcium by increasing active vitamin D and stimulating bone remodeling. It is regulated primarily by serum calcium with some contribution from circulating vitamin D levels.
Parathyroid hormone synthesis, regulation and actions
- Parathyroid hormone (PTH) is a protein hormone synthesized, processed and secreted by the parathyroid chief cells in response to changes in serum ionized calcium levels. Drop in serum calcium levels trigger secretion of PTH via reduced binding to the calcium sensing receptors (CaSR). Furthermore, a rise in vitamin D levels suppress PTH secretion. High phosphate levels also induce PTH secretion by lowering serum calcium and vitamin D levels.
- Parathyroid hormone actions: Major effects of PTH are mediated in kidneys and bone.
- Renal effects
- Increased calcium reabsorption: Stimulates calcium transport in the DCT and the thick ascending loop of henle (TALH) through up-regulation of TRPV5 (calcium channel) and calbindin both directly and indirectly via rise in vitamin D levels.
- Increases phosphate excretion: Inhibits phosphate reabsorption in proximal and distal tubule through endocytosis and proteolysis of sodium-phosphate co-transporters.
- Increases vitamin D production:
- Stimulates hydroxylation of vitamin D by rapidly inducing transcription of 1α-hydroxylase in the proximal tubule
- Inhibits transcription of 24-hydroxylase gene in proximal tubule increasing availability of active form of vitamin D.
- Bone effects
- Stimulates bone resorption: Increases osteoclastic activity through upregulation of RANKL and downregulation of OPG secretion by osteoblasts.
- Increases bone formation: Bone formation increased indirectly via autocrine and paracrine pathways through release of IGF-1, FGF-2 and amphiregulin from osteoblasts.
Calcitonin
- Produced in the parafollicular cells of the thyroid gland, calcitonin acts to correct hypercalcemia by directly opposing the effects of PTH by inhibiting intestinal absorption of calcium, inhibiting osteoclastic activity and inhibiting reabsorption of calcium in the nephron.
Phosphate metabolism
- Phosphate is readily absorbed in small intestine via active transport by sodium-phosphate cotransporters whose activity is increased by vitamin D and an increased filtered load of PO42- and can be reduced by PTH which down regulates apical expression of the cotransporter.
Bone homeostasis
- Guyton Textbook of Medical Physiology, 11e, Ch. 79
- Robbins Pathologic Basis of Disease, 7e, Ch. 26
- Clin J Am Soc Nephrol. 2008 Nov;3 Suppl 3:S131-9.
- Endocr Rev. 2000 Apr;21(2):115-37.
Table 1: Components of bone
|
Origin |
Cells |
Function |
|
Mesenchymal |
Osteoblast Osteocyte |
Bone formation Dormant osteoblast in bone matrix |
|
Hematopoietic |
Osteoclasts |
Bone resorption |
Osteoblast function
- Mesenchymal stem cells within the periosteum, called the osteoprogenitor cells, can differentiate into osteoblasts, following stimulation from the bone morphogenic protein. Osteoblasts have a 3 month life span, then either become osteocytes or bone surface-lining cells. Osteocytes are dormant osteoblasts embedded in the mineralized bone.
- Osteoblasts secrete the components of the bone matrix including collagen and proteoglycans. Polymerized collagen monomers give the bones their tensile strength and the tight binding with the bone salts gives the bone its shear strength. Proteoglycans play a role in bone salt deposition.
Deposition of calcium and phosphate ions
- Calcium and phosphate salts have an intrinsic attraction to the bone matrix through a mechanism that is not well understood. They initially deposit as non-crystalline compounds and are subsequently converted to hydroxyapatite [Ca10(PO4)6(OH)2], the main crystalline salt of the bone. Hydroxyapatite functions to store ions and gives bone its compressional strength. Some of the hydroxyapatite remains in the in non-crystalline form to facilitate a rapid resorption, when needed.
- Pyrophosphate is responsible for inhibiting hydroxyapatite precipitation in other tissues along with maintenance of low physiologic concentrations of these ions. Osteoblasts inhibit pyrophosphate activity in the bone allowing precipitation of these minerals.
Osteoclast (OC) function
- Hematopoietic stem cells can differentiate into osteoclasts, monocytes, and macrophages, all of which express tumour necrosis factor (TNF) receptors.
- Increase bone resorption, in response to physiologic signals (see figure 2 for details)
Receptor activator for nuclear factor κB (RANK) and RANK ligand (RANKL)
- The binding of RANKL to RANK stimulates osteoclast formation, differentiation, and activation (see figure 2 for details).
Osteoprotegerin (OPG)
- OPG is member of the TNF family of receptors that is released by several cell types, including osteoblasts, marrow cells, and immune cells.
- It inhibits the function of RANK by binding to RANKL and preventing its interaction with RANK.
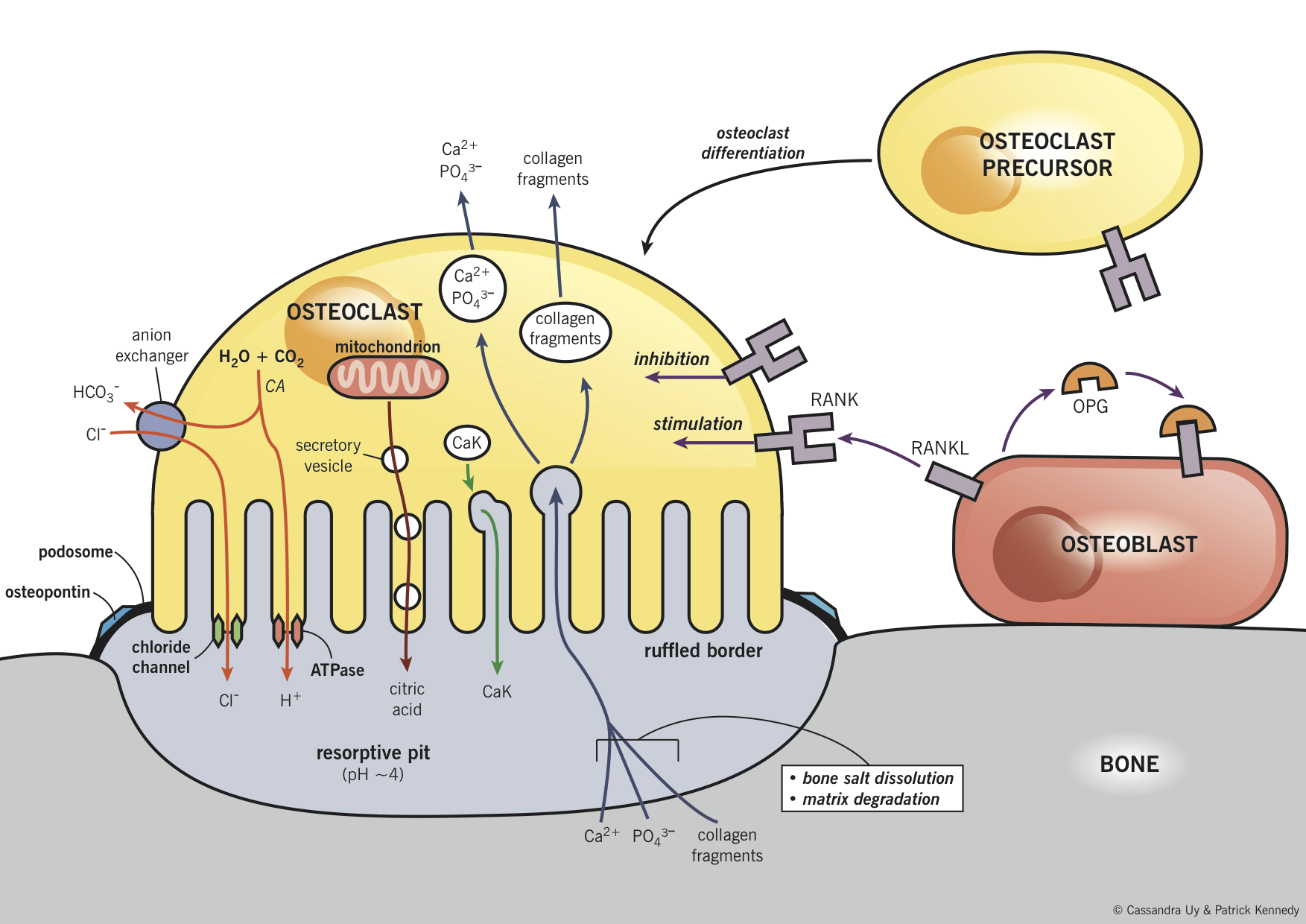
Figure 2: Bone resorption and the relationship between osteoblasts and osteoclasts. RANK is expressed on the osteoclasts, allowing signals from other cell types to affect their life cycle and activity. RANKL is expressed on marrow cells and osteoblasts. The binding of RANKL to RANK stimulates osteoclast formation, differentiation, and activation. Villous projections from an osteoclast form a ruffled border on the surface of bone, which increases the membrane surface area. Podosomes and their associated linking proteins (e.g. osteopontin, meaning “bone bridge”) create an adhesive ring around the ruffled border. This creates a resorptive pit that is sealed off from the adjacent bone and from the ECF, wherein reactions that facilitate resorption occur. Several acids (e.g. citric acid, lactic acid) are released from the mitochondria and secretory vesicles. Hydrogen ions are also released through the actions of carbonic anhydrase and vacuolar ATPase proton pumps. This creates an acidic environment in the resorptive pit, which results in bone salt dissolution. Proteolytic enzymes (e.g. cathepsin K) are released from lysosomes in the osteoclast. These enzymes break-down the collagen bone matrix and are most active in an acidic environment. Materials within the resorptive pit are phagocytosed and moved across the cell and released into the ECF, this results in an increase in ion concentration in the blood. CaK = cathepsin K, CA = carbonic anhydrase. RANK = receptor activator for nuclear factor κB, RANKL = RANK ligand.
Osteoporosis
- N Engl J Med 2003; 348:618-629
- Williams Textbook of Endocrinology 12E
- J Clin Invest. 2008 115:3318-3325
- J Clin Invest. 2000 November 15; 106(10): 1203–1204.
- Eur Spine J. 2003 12:S90-S96
- Endocrine Reviews. 2000 21(2) 115-137
Overview of osteoporosis (OP)
- Osteoporosis is a condition defined by decreased bone mineral density (BMD), resulting from increased bone degradation, decreased bone deposition, or both.
- Any factor that reduces BMD can contribute to or cause OP
Etiology and pathogenesis
- Estrogen deficiency (post-menopausal state) and testosterone deficiency
- Estrogen acts on multiple cells via estrogen receptor (ER) α, with a net result of increased BMD. Therefore, the deficiency of estrogen increases bone resorption, caused by increased OC numbers (due to enhanced OC formation and reduced OC apoptosis).
- Bone cells do not have receptors for testosterone, rather its effect on bone is indirect through the local aromatization to estrogen.
- Insufficient calcium intake
- Serum calcium is tightly regulated by vitamin D and PTH (described previously).
- Insufficient calcium intake leads to secondary hyperparathyroidism, which increases the rate of bone remodelling to maintain a normal serum calcium levels.
- The imbalance between resorption and formation of bone leads to accelerated bone tissue loss.
- Vitamin D deficiency
- Certain populations are at increased risk of vitamin D deficiency, including obesity (due to decreased bioavailability of Vit D), individuals living far from the equator (reduced sun exposure) and the elderly (impaired intestinal absorption and decreased cutaneous production of vitamin D)
- Vitamin D insufficiency also leads to secondary hyperparathyroidism, and accelerated bone loss.
- Physical activity
- Active individuals impose strain on their skeletal system, resulting in microtrauma and appropriate bone remodelling and strengthening.
- Inactivity result in minimal strain and shift in bone remodelling toward osteoclast activity, leading to bone loss.
- Smoking
- Use of cigarettes is detrimental to bone health by multiple mechanisms:
- Tobacco compounds have a direct toxic effect of osteoblasts.
- Estrogen metabolism is altered, leading to earlier menopause.
- Smokers are more likely to have poor exercise habits and a need for medications that may be detrimental to bone health (e.g. glucocorticoids for lung disease).
- Use of cigarettes is detrimental to bone health by multiple mechanisms:
- Illnesses associated with OP
- Certain gastrointestinal disease result in impaired absorption of bone minerals and vitamin D and therefore contribute to OP (e.g. malnutrition, malabsorption syndromes (celiac and crohn’s disease), short gut syndrome).
- In hypogonadal states, there is decreased functional activity of the gonads and the positive effects of estrogen on bone health is reduced (e.g. Turner’s syndrome, anorexia nervosa).
- Endocrine disorders can impair bone health through a variety of mechanisms (e.g. Cushing syndrome, hyperparathyroidism)
- Medications associated with OP
- Glucocorticoids (e.g. prednisone) are the most common cause of medication-induced OP. They adversely affect bone metabolism by multiple mechanisms:
- Stimulation of osteoclast differentiation
- Inhibition of osteoblast proliferation
- Decrease in intestinal calcium absorption
- Increase in renal calcium reabsorption
- Other immunosuppressants, such as cyclosporine, can also cause rapid bone loss through similar mechanisms to glucocorticoids.
- Thyroid hormone directly stimulates bone resorption. Endogenous thyrotoxicosis accelerates bone turnover and is a significant risk factor for development of OP.
- Aromatase inhibitors are used for the treatment of estrogen-dependent cancers of the breast and ovaries. They limit the synthesis of estrogen and can therefore lead to bone loss secondary to estrogen deficiency.
- Glucocorticoids (e.g. prednisone) are the most common cause of medication-induced OP. They adversely affect bone metabolism by multiple mechanisms:
Clinical features
- Patients with low BMD are usually asymptomatic until a fracture occurs.
|
Signs and symptoms |
Mechanism |
|
Fracture (most commonly in mid-thoracic vertebrae, hip and wrist) |
Loss of BMD (see above for pathogenesis) leads to weakening of the bone predisposing them to fractures with minor trauma. |
|
Kyphosis or dowager hump or loss of height |
Progressive vertebral compression fractures. |
|
Fragility fractures (defined as a fracture occurring due to a fall from standing height or less) |
Consequence of the decrease in bone strength and disorganized bone remodelling. |
|
Bone pain (hip, back, pelvic, radius) |
Usually secondary to fractures. |
Treatment
- N Engl J Med 2010; 363:2027-2035
- J Clin Endocrinol Metab. 2011 Jan;96(1):53-8.
- Endocr Rev. 2005 Aug;26(5):688-703
- Clin Interv Aging. 2007 March; 2(1): 55–64
- Calcium and vitamin D
- Circulating levels of both calcium and vitamin D tend to decrease with age due to decreased consumption, impaired intestinal absorption and decreased cutaneous production of vitamin D.
- Calcium supplementation of 1000 – 2000 mg/day is recommended, taken in doses of ≤ 600 mg to maximize absorption, with no significant difference shown between different calcium supplementation formulations.
- Vitamin D, by inducing synthesis and expression of calcium transporters in the intestine and kidneys, should be supplemented in conjunction with calcium at a dose between 400 and 2000 IU/day.
- Estrogen
- Estrogen receptors are found on many cells involved in bone metabolism, with ERα primarily found in cortical bone and ERβ in cancellous bone.
- Net effect of increasing bone density by increasing OPG levels, inhibiting production of osteoclasts from precursor cells and promoting osteoclast apoptosis.
- However, controversy surrounds its use given potential increase in cardiovascular disease and breast cancer and therefore appropriate patient selection must be employed when starting hormone replacement therapy.
- Bisphosphonates
- Bisphosphonates are analogues of pyrophosphates which are compounds naturally found in bone matrix and act by specifically impairing the action of osteoclasts and inducing apoptosis of osteoclasts.
- Bisphosphonates bind to hydroxyapatite binding sites and impair the ability of the osteoclasts to properly adhere to the bony matrix thereby reducing osteoclastic bone resorption.
- Emerging evidence suggests that bisphosphonates also prevents osteocyte and osteoblast apoptosis.
- Alendronate, risendronate and ibandronate are approved for the prevention and treatment of osteoporosis.
- Selective estrogen-receptor modulators (SERMs)
- SERMs alter the ratio of co-activator to co-repressor proteins in different cells and can thus act as either agonists or antagonists of estrogen receptors (ER).
- In bone, agonistic activity on ERα leads to a reduction in bone resorption.
- Currently, two SERMs (tamoxifen and raloxifene) have been shown to be beneficial in the treatment of post-menopausal osteoporosis.
- Teriparatide
- 1-34 or 1-31 amino acid sequence of PTH (physiologically 1-84 AA).
- The first two amino acids are obligatory for biological activity, and it appears that the bone anabolic properties are fully maintained by the foreshortened fragment (1–31).
- Given intermittently, osteoblast activity is upregulated over osteoclastic activity.
- Lifestyle
- Exercise can be effective in preventing bone loss and improving balance, coordination and strength, thereby reducing risk of falls. Thirty minutes of weight-bearing exercise should be undertaken daily by patients who are able to tolerate it.
- Smoking cessation and minimizing alcohol consumption are also beneficial.
- Reducing medications and minimizing dosages, especially glucocorticoids, should be considered.